
I’m doing an experiment with “continuous content” and more stream of conciousness analysis. The piece is set up as a group of different short vignettes that aren’t necessarily related. Check out the central page for more details
Table of Contents
- Inefficiencies of Human Docs
- Tech As A Tool vs. Tech As A Priority
- Healthcare Needs Normal CAC/LTV
- Beating EMRs
- Healthcare’s In Group and Out Group
Inefficiencies Of Human Docs
Let me lob a question out there: If it were technologically possible today, do you think doctors should be fully automated? A large chunk of people would say no, a doctor should always be in the loop at some point in the process or there are benefits to having a human involved in care.
It’s important to remember doctors are human too, and that’s not always a good thing. Some downsides
- Conversations — Human doctors means interactions require social etiquette. That includes idle small talk and conversation as a means of moving information. One of the reasons companies like Lemonaid and Nurx work better is because removing the conversation/face-to-face aspect means you can scale the service and reduce cost. A doctor can “see” significantly more patients in 30 minutes asynchronously than one face-to-face meeting.
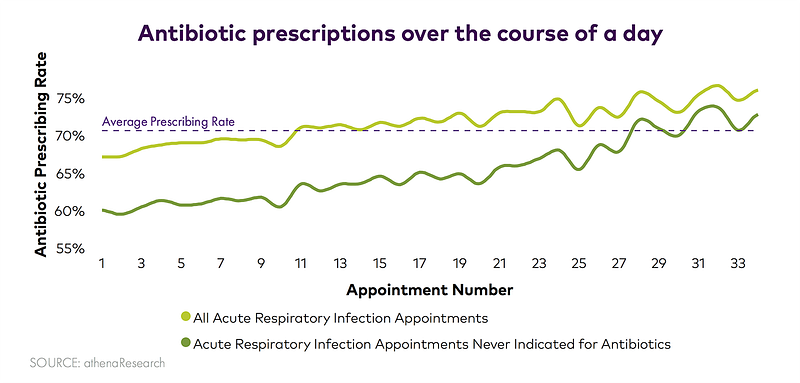
- Fatigue — Sometimes your doctor just wants to go home! It turns out that when you see your doc during the day or the kind of mood they’re in could actually affect their decision making. For example, the later the more appointments a doc has the more likely they are to prescribe antibiotics later. Decision fatigue is real!

- Trust — Human doctors means human judgment. There are certain questions we ask Google that we would never ask another human being. This is true of medicine too — even if we’re supposed to be honest sometimes it’s just embarrassing to do so especially with things like sexual health, substances, or mental health which might carry social stigma. For example, Clue has more detailed and accurate data from its base than what doctors collected.

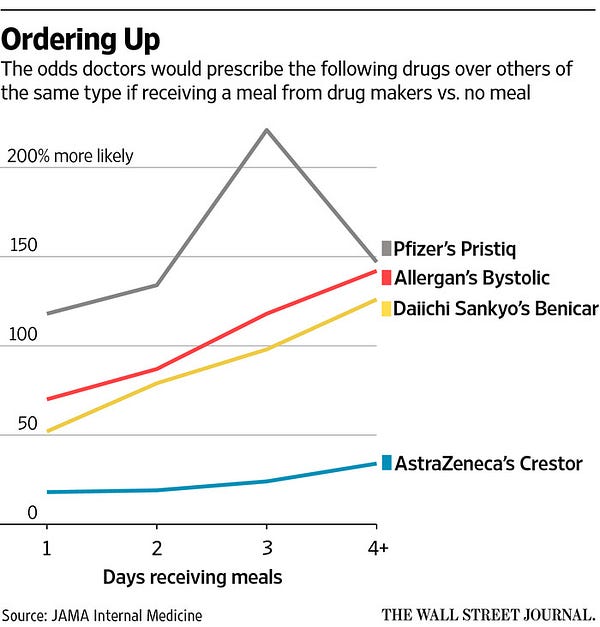
- Influence + Bias — There are things outside of you that influence how a human doctor will think. They care about normal things like money, status, etc. sometimes more than they care about your individual care. Pharma’s cozy relationshipwith doctors is no secret and it influences your care. Same thing with racial bias. It should be noted that automation isn’t a panacea since algorithms are susceptible to the biases of whoever programs it but it’ll at least force us to codify and confront them.
- Updating — Doctors are busy people, they understandably might not have time to keep up to date with all the new research, devices, etc. pushing the industry forward. Computers can be updated and absorb new information much faster.
All this being said, full automation also poses its own risks of course and it’s not even clear if patients want that. But there are so many articles about the promise and negatives of AI in healthcare, yet seemingly fewer on the issues of having a human as your doctor.
Tech As A Tool vs. Tech As A Priority
In the first wave of digital health, we saw a lot of companies build tech tools, hardware, SaaS products, and more with existing incumbents as the buyers.
Turns out there are a few problems with that. Sales cycles are really long, you’re playing in someone else’s sandbox and are dependent on their data, it’s hard to scale because many times you have to do some form of custom implementation or training, etc.
But if you really believe your tool is better and something an incumbent can’t easily build themselves, isn’t there more upside to competing with them than selling to them? I actually think one of the edges new companies have is they are a more attractive place for talented tech operators to work. How many great engineers do you know want to go work for or with the existing healthcare giants? Creating new businesses that puts this engineering and technology paradigm shift at the core of its culture is something healthcare giants will have a hard time doing.
A key premise for the next decade: it’s easier for software to enter other industries than for other industries to hire software people
— Benedict Evans (@BenedictEvans) September 3, 2016
This is why my bet is that the biggest winners in healthcare going forward will be ones that
- Have technology as the central pillar of their strategy and culture
- Generate their own data rather than rely on someone else
- Take as many parts of their value-chain as possible (aka. going full-stack)
An area I see this a lot nowadays is AI — plug-in tools designed to optimize some efficiency, do some analytics, or help find answers faster. But how many plug-in solutions have you seen that scale in healthcare generally? How much time is spent structuring and cleaning data from different sources? Watson, a trusted brand with an enormous sales force, is a case study on the difficulties.
“At hospitals that don’t link it with their medical records, more time must be spent typing in patient information. At Jupiter Medical Center in Florida, that task falls to nurse Jean Thompson, who spends about 90 minutes a week feeding data into the machine. Once she has completed that work, she clicks the “Ask Watson” button to get the supercomputer’s advice for treating patients.”
Watson’s story with MD Anderson also highlights another issue — when things goes wrong, who is to blame? Not owning the full stack exposes a company to failure in things outside of its control. If you believe in your technology, then to maximize it you want to control the inputs and benefit in the full-financial upside if it’s better than the competition.
I expect the next group of successful digital health companies will be competitors to the incumbents as opposed to tools for them, AI included.
Healthcare Needs Normal CAC/LTV
There’s a pretty straightforward metric companies use to measure their marketing spend: Customer Acquisition Cost (CAC)/Lifetime Value (LTV)
Normal businesses have to do things like market to customers, compete on their offerings, and find their most profitable avenues of distribution for CAC. On the LTV side, they have to price their goods and services accordingly and invest in the customer experience to keep people from churning.
Healthcare has managed to dodge this completely. CAC is completely distorted either because consumers choices are made for them and LTV doesn’t exist since churn is dependent on how long you stay with your employer, not your own preferences. The consumer/user and the purchaser are two completely different people. Insurance carriers consider the customer as employers even though the users of the product are patients.
If carriers had to actually care about the CAC/LTV ratio for patients, they’d be way more likely to actually improve the customer experience, invest heavily in preventive programs, and find more ways to keep consumers stick to their offering. You probably wouldn’t need to impose artificial caps like Medical Loss Ratios — where insurance companies have to spend at least 80% of revenue from premiums on paying out claims.
I think this one (of many) reasons that Medicare is one of the most interesting areas in healthcare right now. Since Medicare recipients don’t get their insurance through their employer and each Medicare member is worth a lot of money (very high LTV) — it looks more like a competitive marketplace.
The implementation of the star rating tells both us and the market how good plans are at customer service, managing chronic conditions, preventive care measures and more.
In fact, when we look at the people who do switch Medicare Advantage plans, it tends to be away from plans that are poorly rated.

And that’s just for people who voluntarily choose to switch, most people actually keep their Medicare Advantage plan because they compete for a better customer experience and the plans can invest in the longer-term health of these populations
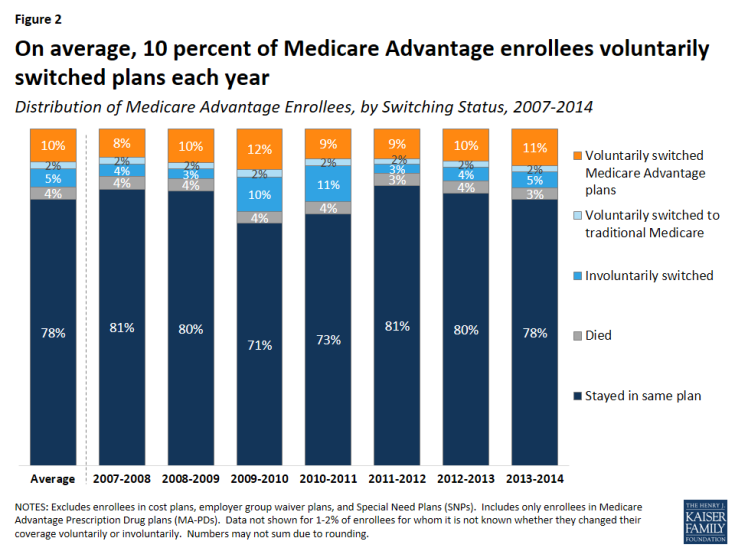
Compare this to employer based markets, where average tenure at a job is less than 5 years and more than 50% of people who change employed-based insurance plans is due to a job switch or employer decision. Why would any health plan choose to invest in the long-term health of a person leaving so soon?
This is why I think decoupling employment from insurance should be a way higher priority — it distorts the CAC/LTV ratio and has become a tool for large companies to lock-in talent. Parts of the ACA aimed to address this with the exchanges, Cadillac Tax, etc. but the fate of those doesn’t seem very promising.
Beating EMRs
I think there’s a reasonable case to be made that the lack of data interoperability that electronic medical records (EMRs) present has been a massive hurdle in pushing healthcare forward. Secure patient info as-a-service to build on top of would probably make everyone generally happier.
Direct competition with EMRs is going to be hard at this point. Hospitals are risk-averse purchasers and these companies are deeply entrenched. So how do we get there? Some crazy and not-so-crazy ideas:
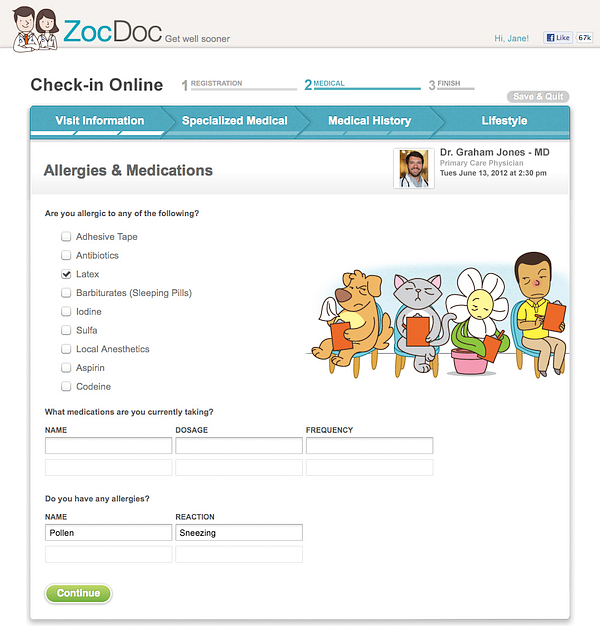
Services that ALSO gather patient data — Certain companies gather data from patients as a byproduct of their service. Zocdoc is a good example of this with their medical history and pre-check in questionnaire. Every time you use Zocdoc, you’re actually building a patient record of yourself. The same thing is true for telemedicine visits, genetics testing, etc. Patients come for the service, but could end up building a personal health record in the process.
EMRs as a public utility — I read this interesting paper about treating money as a public utility that started with this:
Traditional infrastructure regulation — the law of regulated industries — rests atop three pillars: rate regulation, entry restriction, and universal service. These three regulatory techniques are widely deemed appropriate under conditions in which (1) the price mechanism does not allocate a given resource well and (2) broad access to the resource is especially desirable.
That…kind of sounds like patient information to me. Maybe EMRs should actually be a public utility, and innovation in the space should be shouldered by the applications that build on top of it. In fact many of the arguments I hear in favor of Net Neutrality could also apply to healthcare, except healthcare is in the position that it actually needs to fight to GAIN neutrality.
Middleware capture — Right now someone (doctor, nurse, medical scribe, etc.) inputs data into an EMR during a visit. This process sucks, and many hospitals are looking for ways to make this more seamless. One area I talked about in the last installment was voice as a potentially easier way for doctors to input data. Is it possible for this middle voice layer to capture the data and create its own patient record? I’ve thought about this similarly with email and chat clients, where doctors are routinely putting unstructured text data that could form a patients health record.
Blockchain…? I’m going to preface this by saying I’m still wrapping my head around blockchain stuff. While I’m skeptical you can create a blockchain-based health record out of thin air, shifting data governance to patients instead of centralized entities seems like an inevitability. It’s pretty weird that everyone but the patient holds the data, even if the patient owns it. I mean you have to pay for a copy of your own data, what???

Plus the fact that patient data is so valuable and patient services are so expensive creates an opportunity to incentivize patients to give their data. I’m curious about the doc.ai model for example, which uses tokens to incentivize people to give their data to training models that improve their healthcare chatbot service. The whitepaper is an interesting read.
Healthcare’s In Group and Out Group
More anecdotal than analysis. I’m always shocked at how eager people in the healthcare ecosystem seem to be to scoff at tech companies.
People deep in healthcare seem to pride themselves in how long it’s taken to build their knowledge and expertise, and therefore the only people who know how to change the system is them. There’s a general wave of sentiment when a tech company tackles a problem of “they really don’t have a clue what they’re getting themselves into” and an “I told you so” smirk when a tech company shuts down.
I feel like the trope that “tech founders are arrogant about fixing healthcare” is overblown today, most serious entrepreneurs respect how hard healthcare is. The smugness of people deep within the health system when a new entrant comes in is misplaced— everyone in this space is on the same team of trying to lower cost and improve outcomes.
We should be doing everything possible to make healthcare a place more people want to innovate in. Of course bad actors should be called out, but it benefits no one to be condescending. Being thoughtful and explanatory is better than smarmy.
My goal is to write about healthcare in a thoughtful and approachable enough way that people don’t feel intimidated in getting involved in the space. If you’re truly knowledgable and want things to change, that should be your goal too.
If anything I wrote in my stream of consciousness resonates with you, please reach out to me on twitter @nikillinit, and I’d love to hear your thoughts.